Case 1 180706-1 (18N1093)
Conference Coordinator: Dr Melissa Roy.
//
Three-month-old, male, Knabstrupper colt.
The owner first noticed the colt to be non-weight bearing lame in the right, front limb ten days prior to presentation. At that time the owner did not appreciate any heat or swelling and noticed that the foal was nursing normally and seemed bright. Four days later the foal was dull and lethargic. Several hours later the foal appeared to be improving. This morning the owners found the foal laterally recumbent and described it as cold and unwilling to stand or nurse. The owners were able to help the foal to stand but noted that it was unstable and standing with its head and neck twisted back.
On physical exam, the colt was febrile (104.4 F), non-weight bearing on the right front limb, and dragging right front toe. He appeared slightly contracted in both hind limbs. Radiographs showed a 1.1-cm-diameter lucency in the right distal humeral physis. Ultrasound examination of the right proximal antebrachium and humeroradial joint showed a pocket of fluid of mixed echogenicity adjacent to the bone. The pocket extended to the medial aspect of the limb and around the physis. These findings were interpreted as moderate synovitis with multifocal anechoic fluid pockets. Joint fluid was collected aseptically and submitted for cytology, which revealed marked suppurative inflammation. Culture of the fluid grew Streptococcus equi subsp zooepidemicus. The colt was euthanized due to poor prognosis.A 155-kg, 3-month-old Knabstrupper colt was necropsied. There was a moderate amount of swelling over the right elbow joint. A large amount of yellow, fibrinous and gelatinous, malodorous material filled the joint space, and dissected through gravity-dependent tracts along fascial planes and between muscle bundles. Longitudinal section through the humerus revealed an irregularly demarcated, 1.0-cm-diameter lytic lesion extending through the epiphysis, physis, metaphysis, to the caudal aspect of the cortex.
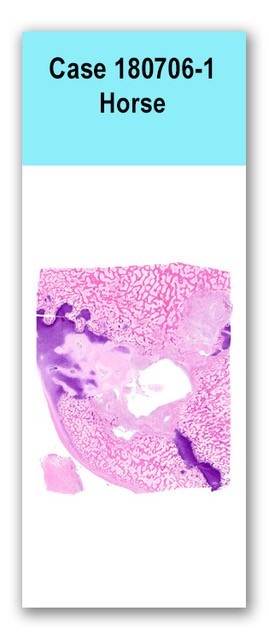
This slide has one cross section of bone at the level of the physis, in which the central 60 to 70% of the physeal cartilage is necrotic, cavitated, and disrupted by a dense aggregate of inflammatory cells, including large numbers of neutrophils with fewer macrophages and lymphocytes, and plump, reactive fibroblasts. The inflammatory population also infiltrates into the adjacent epiphysis and diaphysis, disrupting normal trabecular architecture and filling medullary cavity spaces. Cartilage and bone within the inflamed region are fragmented, disorganized, and variably necrotic. Bone spicules have scalloped edges lined with numerous osteoblasts and fewer osteoclasts in Howship’s lacunae (bony remodeling). Surrounding the dense physeal inflammation is a thin lattice of woven bone. Adjacent trabecular bone retains cartilaginous cores. The superficial surface of the articular cartilage is necrotic, and the synovium is infiltrated by large numbers of plasma cells, lymphocytes, and neutrophils. A section of presumed joint capsule is also on the slide, and is infiltrated by a similar inflammatory population.
A Gram stain was performed on the section, but no bacteria were observed.
Distal humerus: Focal, suppurative osteomyelitis and physitis with bony lysis, cartilage necrosis, and regional fibrinosuppurative and necrotizing synovitis, capsulitis, and arthritis
This lesion was most consistent with an embolic or septicemic process, due to the subjects you age and the location of the physeal abscess and osteomyelitis. The synovium and surrounding joint were also severely affected with the fibrinosuppurative exudate and the synovium was partially necrotic. It is unclear whether these are two separate processes (arising independently from the embolic episode), or if there was a physical connection, such as a physeal abscess, which extended outward into the joint. It is also possible that the joint was affected first and spread into the bone, but this is considered less likely given the focal distribution of the physeal and metaphyseal lesion and the relatively intact articular cartilage. Joint fluid submitted clinically for culture revealed Streptococcus equi ss zooepidemicus, which has been implicated in septic arthritis and septicemia in foals, particularly in older foals (Hardy, 2006). We thank Dr. Kevin Woolard for contributing this case.
Hardy J. Etiology, diagnosis, and treatment of septic arthritis, osteitis, and osteomyelitis in foals. Clinical Techniques in Equine Practice. 2006; 5(4): 309-317.
Conference presenters: Drs. Melissa Roy and Brian Murphy